

Where Do You Land When Your Mind Falls Apart?
Liisa suffered a nervous breakdown. She was transported to the emergency room at UP Health System Portage.

Editor’s Note: Some last names have been omitted to protect the privacy of the individuals.
Liisa suffered a nervous breakdown. She was transported to the emergency room at UP Health System Portage.
“Because there are no psych beds or a transitional holding area to be assessed in our area, I was placed in a small broom closet off the main room,” she recalls. “It had no windows and harsh lighting, and it was claustrophobic.
“I was there many, many hours while the hospital was waiting for a bed to open up at Marquette General or elsewhere.”
Brett went off his psych meds and became manic. Instead of landing in a local emergency room, he went to Northland Counseling’s crisis house in Ashland, Wisconsin.
“It was a friendly and warm home,” he says. “In some ways, it was much better than my own living situation at the time. It had all the benefits of a hospitalization, but was more comfortable. The workers were responsible, kind, and much less stressed-out than at a hospital. We were allowed outside to play in the grass or talk or just smoke once an hour, which also kept the stress lowered for nicotine addicts like myself.
“It was a nice way to start taking better care of myself, and just to remember what a healthy, normal lifestyle is like.
“I think something like Northland Counseling Crisis House would be great for the community in this area. People with less serious crises could go there, if even just to wait for a hospital bed to open up somewhere else—instead of staying in an ER room. It would definitely be a major improvement.”
Liisa agrees.
“There is a pressing need for something like a transitional/assessment/holding house or center for immediately after a person in crisis is brought to an ER and for the next 12-24 hours or so,” she says. “Somewhere a person could be attended to while doctors or other professionals can figure out the best course of action for the patient. Perhaps in a softer, less sterile, less harsh, less intimidating atmosphere. I believe this would be beneficial for a patient who is already under duress psychologically.”
No Crisis Center Here

Sheriff Josh Saaranen
The Keweenaw has no such place where people in mental health crisis can go and feel safe, comfortable and cared for while awaiting further placement or referral. Houghton County Sheriff Josh Saaranen says that local law enforcement responds to mental health-related calls on an almost daily basis.
Sheriff Saaranen likes the idea of a crisis center.
“While some individuals need long term care, many people in crisis need short term solutions,” he says. “A crisis center could offer an opportunity for these individuals to stay within our community. It's healthier for the person to be closer to their family and or support groups.
“Individuals are often placed in treatment centers throughout the state,” the sheriff said. “Oftentimes we see these individuals stay in these centers for a couple of days and be released; they then have to arrange transportation back home. I can imagine that this is a stressor that a crisis center could alleviate.
“This would also be safer and healthier for the sheriff's office staff,” Saaranen says. “These trips require two deputies and tend to be long drives in all types of weather. A short term crisis center would aid in limiting these strenuous trips for the patient and deputies.”
Data compiled by Copper Country Community Mental Health (CCCMH) showed that nine people have had to stay in an emergency room for two days or more since October 1, 2022.
“CCMH is very concerned about the problem of multi-day ER assessments,” says the mental health center director, Mike Bach.
A crisis center could serve as a step back into community for people coming out of the hospital, a short-term stabilization setting or a site to await placement instead of waiting in the emergency room.
Pressing the Portage Health Foundation
Mental health support and advocacy groups in the area are working with the Portage Health Foundation (PHF) and CCCMH on the need for such a crisis center. PHF is planning a new “wellness campus” in the Keweenaw. The Mental Health Support Group-Keweenaw Area and Keweenaw Support 4 Healthy Minds are urging the foundation to include a mental health crisis center in the facility. Liisa, Brett, and several other mental health clients and family members have written letters to PHF in support of such a center.
Dr. Michelle Morgan, head of Keweenaw Support 4 Healthy Minds, wrote: “As a psychiatrist (now retired) for the local community mental health center, I witnessed the suffering of people in acute mental health crises as they languished in the emergency room for days while waiting for an inpatient bed to become available somewhere in the state of Michigan. With staffing shortages across the country, I know this situation has become all too common. Our rural community is particularly vulnerable, having limited resources as it is.
“A mental health crisis unit is a lower cost and possibly more effective alternative for patients who need increased support and supervision while they engage in treatment with local providers. Rather than being sent away to a hospital, they would benefit from the continuity of care locally, as well as the support of people who know them well. Such a resource could be key to preventing a mental illness from reaching the point where the person might become dangerous to themselves or to others.
“I hope the Portage Health Foundation finds this idea compelling enough to support it.”

PHF Executive Director Kevin Store
PHF has made no decision, but “everything is on the table,” according to Executive Director Kevin Store.
“This is a complex issue,” he says. “PHF is just one party engaged in finding solutions to these issues. The community needs to find ways to work together.
“PHF recognizes the need for a complementary model of mental and behavioral health services that helps meet the needs of all our community members,” Store goes on to say, “whether that be increased education/prevention services, expanding the availability of more acute, short-term counseling services, and finding ways to improve access to mental and behavioral health assessment and referral into the appropriate care.”
“There are many challenges to this issue,” Store adds. “Staffing to appropriate levels with the appropriate training that meets requirements; financial viability and the lack of adequate reimbursement for not only the clinical treatment services, but also to cover administration and support; complex licensing regulations, service provider credentialing, to name a few. All contribute to the complexity of this issue.
“There are a lot of folks and organizations in our region working on trying to find solutions to the needs that exist in our area,” Store goes on to say.
Dr. Kelly Mahar, psychiatric residency director at UP Health System-Marquette, is heading a UP-wide effort to assess and address the mental and behavioral health shortfalls across the UP.
“Like them, PHF is working with a number of partners to seek solutions to these issues. PHF will continue to advocate on behalf of those providers who are working to try to meet the needs,” Store says.
The PHF wellness center is in its early planning stages, Store points out. The foundation has reached out to the community for input and plans to release a report on its findings in April.
Dial Help Anticipates Challenges
Dial Help, which operates a crisis hotline, has some reservations about a mental health crisis center.
“It could be helpful in theory, but the amount of staffing and resources that would be needed is probably prohibitive at this time,” says Rebecca Crane, director of Dial Help. “Typically, something like that would have to have 24/7 staffing, potentially including medical personnel and law enforcement or security. You'd essentially be recreating an ER outside of the supports of an ER. Additionally, people might not utilize something like this due to stigma and fear of being sent to an involuntary psychiatric hold, having their children removed, or friends, families, coworkers finding out that they went.”
Crane says that the number of mental health crisis calls that Dial Help receives are down because there are so many specialized crisis lines now.
“Our numbers have really dropped, not because there are fewer people in crisis, but because they're reaching out to the specialized lines for their specific issue,” she explains.
There are still a lot of mental health challenges in the Keweenaw, Crane goes on to say.
“There is a lack of psychiatrists, lack of counselors in general, lack of mental health treatment options for youth, lack of funding for Copper Country Mental Health, poverty, lack of transportation to get to appointments in our large, rural service area, lack of childcare to attend appointments, difficulty accessing care due to insurance requirements, and there is still a lot of stigma around discussing mental health that prevents people seeking help until things get dire,” she says.
Copper Country Community Mental Health in the ER

CCCMH Director Mike Bach
CCCMH is trying to address those challenges. The mental health center contracts with two residential crisis centers downstate, but because placement is voluntary, patients have to find their own transportation there. The center’s case managers, therapists, and peer support partners try to help people resolve problems before they become a crisis, says Mike Bach, CCCMH director.
The community mental health center does crisis screening in the ER.
“If someone presents in the emergency room in crisis, we talk with the person, friends and family, medical staff, law enforcement and other concerned parties to determine whether safety planning is appropriate,” Bach says. “If a person can safely return home, we arrange follow-up with the person’s treatment team if they are a current consumer. This follow-up may include more frequent contacts and medication adjustments. If they are not a consumer, we help with a referral to this agency or private providers as is appropriate.
“When a person is in the emergency room for multiple days, we work with hospital staff to help that person stabilize and possibly avoid the need for psychiatric hospitalization,” Bach goes on to say.
Two local hospitals are contracting with companies that provide psychiatric consultation to emergency room doctors, Bach says.
“The hope is that appropriate psychiatric treatment can begin in the emergency room, so that the patient can stabilize and possibly return home with a safety plan,” he explains.
Another alternative is EmPATH (Emergency Psychiatric Assessment, Treatment and Healing), a specialized hospital-based mental health emergency unit. There are EmPATH units in a number of hospitals nationwide, but no plans to establish one here.
There are serious challenges to creating a stand-alone crisis center. The State of Michigan has tightened licensing laws, and staffing with qualified medical professionals is difficult in the UP.
“A huge challenge is adequate staffing, which includes psychiatric oversight, medical staff, clinical staff, security, and direct care staff,” Bach says. “Also needed are staff to maintain the building, purchase food and supplies, track staff training, and ensure appropriate IT support.”
Staffing presents one big obstacle. Another is creating a facility offering services that Medicare and Medicaid will pay for.
“If the services provided by the crisis center are billed to Medicaid or other insurance companies, it will need to comply with accreditation requirements and the myriad of regulations required by Michigan and federal laws and administrative rules,” Bach points out.
He says CCCMH is working with many community partners to address issues with mental health crisis care.
“We are very thankful for our local partners and see them as essential for our community to care for those of us who are the most vulnerable,” Bach adds. “We will continue to partner with them as we seek a community solution to multi-day emergency room stays.”
UP Health System-Portage Relies On Partners
UP Health System-Portage spokesperson Alexis Jacques says that the hospital depends on community partners such as CCCMH.
“We are proud of the partnerships and working relationships we have with these organizations and rely heavily upon their expertise and engagement,” Jacques says. “While we understand that behavioral health patients may present to our emergency departments initially, our staff is trained, and resources are available to stabilize a patient so that we can properly establish the best and safest plan for the patient in need.”
Mental Health Advocates Making Waves
Cindy Harrison, a mental health activist and member of the Mental Health Support Group-Keweenaw Area—which used to be the Keweenaw chapter of the National Alliance on Mental Illness (NAMI)—recently wrote a letter to the Portage Health Foundation urging them to consider including a mental health crisis center in their new wellness campus. Houghton County Sheriff Josh Saarinen, whose deputies regularly deal with people in mental health crisis, endorsed it. So did Gail Ploe, prevention specialist and alcohol and drug counselor at the Western UP Health Department, Bill Fink, whose daughter deals with mental health issues, and John Ruuonen, a mental health client and author.
“I can speak to this as the mother of two severely mentally ill children,” Harrison wrote. “I have been dealing with mental illness in the family for twenty years.
“Although this community has many resources in health care, one of the major things we are lacking are resources in mental health. Twenty years ago, Marquette General had a capacity of 24 psych beds and the Soo had over ten. Those numbers have shrunk today, and even with the new UP Health System-Marquette, there are only 12 psych beds being used now, even though the new hospital announced that it was planning for 48 psych beds. We do not have Westside in Calumet anymore, and the Rice House is not being used for crisis care as it once was.
“So, of course, in a psych crisis, more time is being spent in our local ER trying to find a hospital bed anywhere in the state. Sometimes this takes more than a few days, which is extremely hard on the staff and terrifying for the patient and family. Although it would be great to have psych beds available locally in Hancock, this does not seem possible, so the next best thing would be a ‘crisis center’ where people could go for short term care until a hospital bed is found or a place to go after getting out of the hospital when transitional care is needed before coming home.”
Harrison has been to the Ashland Northland Counseling Crisis House.
“It is wonderful, so therapeutic,” she says. “If we could get something like a crisis house for the mentally ill who are having psychiatric problems, that would be a wonderful addition to our community and the western U.P.”

Interacting with the police
For someone with a mental health problem, any interaction with police can be dangerous for officers and individuals alike.
If a police officer is interacting with someone they believe to have schizophrenia, autism, dementia, or numerous other illnesses and disorders, there are special considerations for them to keep in mind.
An otherwise calm person with autism may react violently to being touched after not responding verbally to an officer’s questions.
A person with untreated schizophrenia may have difficulty focusing on the conversation and respond with rambling and difficult-to-understand answers.
Someone with unaddressed depression may be intent on self-harm and lash out at others who try to interfere.
These are just a few of the ways that a mental health disorder can complicate an interaction with police officers.
Despite the chaos it can sometimes cause, being mentally ill is not a crime. However, sometimes those who are mentally ill get treated harshly by those who don’t recognize their mental illness or mistake it for drug abuse or simply bad behavior.
Over the last decade, local police have been working to train themselves on how to better handle the people they interact with who may have a mental illness.
Lt. Nick Roberts works with the Houghton Police Department. He said larger police departments will have specialized social workers working within them but HPD is too small for that kind of specialization. He said that when they have the chance, they do arrange to have the appropriate social worker in the car from CCMH, Dial Help, or elsewhere. They already communicate and work together almost every day with those workers. But when an emergency call comes into 911, time is of the essence and they don’t usually have the opportunity to connect.
“If we have time, great!” Lt. Roberts said. “I’m more than happy to have a social worker come and assist us. They’re just not on our payroll sitting in the seat next to me.”
Additionally, in a bad situation, a social worker in the car could be one more person’s safety an officer has to consider before acting. One reason their universal presence isn’t desired. There are also many calls officers respond to where the social worker is not necessary, so their time would be wasted by constantly riding along.
Lt. Roberts thinks officers are better trained than many people think. He said a lot of the training and improvements that people ask about are already underway, including training on how to better handle situations where a mental illness is involved.
“It’s called Managing Mental Health Crisis training,” Lt. Roberts said.
The training was developed in association by NAMI, MDHHS, and MCOLES (Michigan Commission on Law Enforcement Standards).
Normally an in-person and hands-on class, during the COVID-19 pandemic it has been offered virtually using video conferencing. Lt. Roberts said that actually benefits officers in rural and remote areas like the Upper Peninsula, as it gives them access to distant training that isn’t always affordable for smaller departments because of travel and staffing.
“I feel we’ve come a long way with that training,” Lt. Roberts said.
Officers in the training are not taught to spot and diagnose a mental illness, but they do learn telltale signs of different ailments and disorders. They’re also taught how best to interact with those in the midst of a mental health crisis in order to get a more positive outcome.
He said a big part of the training is drilling officers to remain calm and consider their word choice, mannerisms, and body language.
“They [a person of interest] will watch what you’re doing,” Lt. Roberts said. “If I look like I don’t care, they’ll key into that.”
Lt. Roberts is now a certified trainer in the MMHC curriculum and regularly offers the training to other area departments. He teaches the two-day course alongside a social worker.
“We do our best to get trained and educated,” Lt. Roberts said.
Unfortunately, the method isn’t perfect, and there are shortcomings and limitations that lead to bad outcomes. The first limitation is, of course, getting the training to the officers, which takes time and funding that isn’t always available.
Beyond that, officers still have a primary duty to react to unsafe situations. If a person is armed, particularly with a firearm, Lt. Roberts said they have to treat it primarily as an armed-person situation before they can address any mental illness issues in play. This means securing the area and ensuring officers do everything possible to disarm the person before they can hurt themselves or anyone else.
“We deal with a lot of people who can be suicidal,” Lt. Roberts said.
Roberts said that maintaining a calm attitude and talking through the situation has led to several good outcomes he’s not sure would have been possible otherwise.
Matt and Nola Olson have guardianship of their adult daughter and care for her in their home. She’s been diagnosed with schizophrenia, anxiety, depression, and obsessive-compulsive disorder and is unable to live independently.
“Even though we’re [her] guardian, we don’t have the legal right to restrain her,” Matt said.
So when her diagnosis and medication were still being established several years ago and she had violent episodes, they had to call the police to restrain their daughter and protect themselves.
Matt recalled one time when their daughter was just 14 or 15 years old, they had to call the police because she was wielding a knife and making threats.
“They are being trained to go about it differently,” Matt said. “But at first it was just like ‘Oh, bad things happen, tackle, handcuff,’ you know, just — it was horrible.”
Since they live in a rural area, the Olsons usually interacted with the Houghton County Sheriff’s Department.
It’s been years since the Olsons’ last experience with the sheriff’s department. Matt said they “thankfully” haven’t yet had an experience with the “new and improved” sheriff’s deputies since they’ve received Managing Mental Health Crisis Training.
They said the one time they dealt with the city of Houghton’s police department was a much different, more sedate, and preferable experience.
“I just want people to realize that we’re doing our best,” Lt. Roberts said. “And don’t be afraid to talk to us.”

Pandemic safety procedures leave some mental health patients feeling abandoned
Teletherapy is popular among many of CCMH's patients, but not all of them find it adequate.
Handling the COVID-19 pandemic has been tumultuous for all of us, involving quick adaptation and frequent discomfort. But for those managing a chronic condition like a mental illness, the pandemic created a fog of uncertainty and new barriers to care that exasperated some issues, despite the best efforts of local workers to mitigate them.
The state deemed mental health services essential, so they could continue under lockdown, but they weren’t specific about what preventative measures providers should or could take.
Copper Country Mental Health, the needs-based, government-supported provider of mental health care in the Keweenaw Area, received some basic guidance from the Michigan Department of Health and Human Services (MDHHS), which they combined with guidance from the CDC and the Michigan Occupational Safety and Health Administration (MIOSHA).
“So we had input from a lot of different agencies and organizations, and then we met as like a safety committee, and that involved our nurses, and we developed the protocols,” CCMH Director Cari Raboin said.
Month by month through the pandemic, the guidance they received changed, and so the committee met repeatedly to update their procedures.
“So it was a moving target,” Raboin said. “It was moving and changing all the time.”
The CCMH staff were also concerned because some studies being released showed that severe mental health disorders could be an increased risk factor for mortality in patients with COVID-19. They felt that the increased risk to the people they’re meant to serve called for a higher level of caution.
Therapy was moved to phone or video interaction. Injected medications were offered in the parking lot by masked and gowned nurses. Even emergency room mental evaluations for people brought — sometimes involuntarily — to the hospital were done over the phone in coordination with emergency room staff and family when available.
“[CCMH] staff would talk with them [the hospitalized] on the phone, too,” Raboin said. “So we got a lot of input, more than just the phone assessment.”
Assertive Community Treatment, which is regular one-on-one activity between a patient-consumer and a CCMH worker and often involves things like making and attending appointments or doing personal shopping, was able to continue with some extra precautions.
But any kind of group social activity had to be ended and didn’t resume for a long time. In the best of cases, these activities moved to a virtual format.
Matt and Nola Olson said that was hard on their adult daughter, who also lost the job shredding paper she had been working a couple of hours per week because of lockdown.
Their daughter doesn’t like cameras and so virtual options don’t suit her.
“When everything shut down and isolation came, you could really see it,” said Nola, their daughter’s full-time caretaker.
This in turn meant Nola had less time for her own work and personal care, which were already limited by the lack of trained, available respite care.
“I had to keep her busy,” Nola said.
Nola felt that the isolation was causing their daughter’s symptoms of schizophrenia to worsen. They felt the first therapist they worked with remotely didn’t understand and wasn’t listening to their concerns.
“We have to deal with it, they don’t,” Matt said. “They’re on the other end of the phone.”
The Olsons were able to change therapists to one they felt took more care to compensate for the shortcomings of telehealth, but still feel their daughter would be better served by in-person therapy sessions.
Raboin said there are pros and cons to using teletherapy. Not being able to read physical cues and body language is definitely a drawback, but she said they got a significant amount of positive feedback from consumers about teletherapy, as high as 70% approval in a survey they sent out. Those who have trouble keeping in-person appointments because of transportation issues, or symptoms of their illness that make going out in public more difficult, found it particularly helpful.
“We hope to be able to continue to provide that as an option,” Raboin said.
It’s currently allowed under special federal and state rules, but may not be in the future. Until CCMH hears from agencies that are above them in authority, they can’t make any long-term plans, either. And not having a plan to offer their patient-consumers keeps everyone apprehensive.
The Olsons said that not knowing what the plan was, and not having any direct contact with therapists or other professionals has left them feeling out of the loop and abandoned.
Raboin said communicating was “definitely” a challenge. They sent out letters, updated their website, and attempted other outreach with each update.
“But the best way we found to communicate with people is one-on-one,” Raboin said.
The most reliable way they found to communicate information was to have someone’s case manager or primary clinician talk with a patient-consumer or their guardian directly about new information or changes.
Whereas transportation to appointments is a barrier to care for some, access to broadband internet or wifi is a barrier for others.
CCMH provided iPads for some consumers who didn’t have a good device for video chatting and bought calling cards for others who had limited minutes on their phones.
The Olsons have to rely on dial-up internet or cell-based internet because of the rural location of their home and their financial constraints, which is another thing that keeps video conferencing from being a good option for their daughter, so they mainly rely on audio-only phone therapy.
“As far as mental health was concerned, it’s all telephone,” Matt said. “And it’s hard to gauge things off a telephone… you’re missing all of the visual cues.”
The Olsons said that the double-standard between physical and mental health was part of what made it so frustrating.
“What burnt me up was the hospital was open the whole time,” Matt said. “Granted you had masks and you had to check for fevers and you know, but if you broke your arm you knew you could go to the emergency room and have your arm dealt with.”
But for mental health issues, there was nowhere open to them.
The Olsons are told their daughter has an illness of the brain and it should be treated as a physical ailment, “but we weren’t treated that way.”

Relying on One Another
People needing support, either in their struggle with mental illness or with helping a loved one, turn to the Mental Health Support Group of the Keweenaw Area.

If you’re struggling with your own mental health or a family member’s illness, you have to deal with extra appointments and supervision, finances and expenses, maybe even jail visits and court appearances, and more.
Most people have a personal support network, but for the unique problems a mental illness can present, a more educated, experienced, and patient ear is helpful but can be hard to find. Ones that understand the sensitivity and stigma associated with the illness and experiences can be even rarer.
One place those are freely available is at the Mental Health Support Group - Keweenaw Area, or “not-NAMI”, as the members sometimes call it. The group used to be a part of NAMI, the National Alliance on Mental Illness, and many of its members still are individual members under the Alger/Marquette NAMI group, but heightened requirements and lowered membership caused the Houghton group to give up its national affiliation in 2018. Determined to continue supporting each other, they reorganized as an independent support group.
Several regular group attendees agreed to interview with me, and I was able to attend part of one of their confidential meetings.
“NAMI is a wonderful organization,” Catherine Paavola said.
Paavola is a regular attendee at the MHSG-KA meetings, has a degree in school psychology, and is also a board member with Copper Country Community Mental Health. Her adult son was diagnosed with schizoaffective disorder with bipolar disorder in his mid-twenties and has struggled with the illness for more than a decade.

She said she prefers the term “brain illness” to mental illness.
“Nobody can tell me where their mental organ is,” Paavola said.
She said what the MHSG-KA offers is a place you can “actually pour your heart out…” without judgment, and without people tiring of hearing about the same recurring problem. Paavola said other maladies people usually either recover from or die from.
“Brain illnesses aren’t like that, they’re forever,” she said.
She said the support group can’t always offer help, but they can offer suggestions and encouragement.
“We pray for one another, you know,” she said. “But the most important thing is, we listen.”
One group participant agreed to speak with me but wished to remain anonymous to protect future employment opportunities in the face of stigma against their schizophrenia and obsessive-compulsive disorder diagnoses.
“I’m very fortunate, actually, to be fairly high-functional,” they said. “I hold down jobs, I manage my finances and other responsibilities, I engage in social situations.”
Other than the MHSG-KA, they also maintain a good support system of friends and, using coping techniques and medications, have learned to mostly manage as an individual.

Nonetheless, they see the value of support groups like MHSG-KA and even host other small, virtual groups in conjunction with the Schizophrenia Alliance.
One shortcoming of support groups in the pandemic was their reliance on streaming technology to overcome physical distancing requirements. Rural participants on unstable connections didn’t feel fully included.
“The video is in and out and the words are garbled…” Matt Olson said. “It’s better than nothing, but it’s not much better than nothing.”
Matt and Nola Olson have guardianship of their 20-year-old daughter, who’s been diagnosed with schizophrenia, anxiety, depression, obsessive-compulsive disorder as well as some other general health issues. She sat nearby listening as I spoke with her parents.
“I’m not going to say our daughter has the worst case, but it’s pretty severe,” Matt said.
They’re happy to have her at home and that she’s being cared for by people who love her, but they don’t feel they get the support they need to make it truly work well. One thing they find is particularly lacking is the availability of respite care for Nola, who cares for their daughter almost all day, every day while Matt works as a well digger to support the family.
“She’s still our daughter, we love her very much, but there’s a point where most people, their children are having lives of their own,” Matt said. “And we’re not there yet, and it creates a lot of stress.”
To care for someone with their daughter’s needs requires someone with considerable knowledge and training, and while members of MHSG-KA are supportive, most of them don’t have that experience, and not all of the Olsons’ extended family is understanding or supportive.
“My mom came around, and she does help us,” Matt said.
However, his mother is getting elderly and can’t help out for very long, or for overnight periods. Nola has recently been diagnosed with fibromyalgia, which her doctor believes is stress-induced.
The Olsons do like attending in-person MHSG-KA meetings when they’re available, saying it’s an “awesome time for sharing, for support.”
Another problem with the groups is trying to get the word out. Paavola said they’ve received little response, let alone support, from local healthcare offices, and the Olsons, who are interested in a schizophrenia-focused respite care group, don’t have a way of contacting other families who might want to join them.
CCCMH and other health organizations and state agencies might have that information but HIPAA law prevents them from being able to share it with group organizers without gathering permissions from each individual.
The “not-NAMI” group has recently resumed meeting monthly, in person, where they share round table discussions about themselves and their loved ones. You can contact the Mental Health Support Group - Keweenaw Area by emailing MHSGKA@aol.com.
Autism advocates pushing for greater awareness, understanding in others
“If you’ve met one kid with autism, then you’ve met one kid with autism,” said Janel Summers, the autism consultant at the Copper Country Intermediate School District.
Mental Health Support Series, Part 2
Autism is a developmental disorder that can be uniquely challenging because of the variety of behaviors and symptoms associated with it.
“If you’ve met one kid with autism, then you’ve met one kid with autism,” said Janel Summers, the autism consultant and special education instructional coach at the Copper Country Intermediate School District.
Summers said that Autism Spectrum Disorder now also includes several diagnoses that used to be considered separately, including Asperger's syndrome, and pervasive developmental disorders.
Some of the things most commonly associated with autism are difficulties with communication and social interaction and certain repetitive behaviors, but it can vary greatly from person to person, as autism is diagnosed on a spectrum.
“Some kids become very social outside,” Summers said, as an example.
Others might do better in music class, or in mathematics. Some might not present with any obvious symptoms. Summers described an autistic person’s skills as a line with mountaintops on it, or “hills and valleys”. And each person with an autism diagnosis has a different set of those hills and valleys.
This can make supporting people with autism especially difficult because each support system has to be individually crafted, there is no universal, or even a typical, option. Summers said that they have to meet people with autism in their usual environment and learn about them to see what kind of supports would be helpful for them.
The number of people with an autism diagnosis has been growing, according to statistics from the Centers for Disease Control and Prevention, but it’s unclear if that is because of advances in detection or an actual increase in people with the disorder. Summers said it’s more commonly diagnosed in boys, to a 4-1 ratio, but it may be due to boys' tendency to show more outward aggression that makes it easier to identify.
Autism Supports in Schools, and Beyond
Autism in education has changed. Once, special education classes kept students diagnosed with autism and other disorders apart from regular lessons with other students. Now —
“Our goal is to have 80% of our students in gen-ed [general education] 80% of the time,” Summers said.
Rather than grouping students with autism together into special education classes, the goal is to give them what support they need to succeed in the same environment as other students. Summers said a large part of this is the goal to avoid removing them from the social environment of the classroom, which is as important for them as any other student.
Supports like social stories, visual schedules, sensory tools like weighted blankets, and video models of behavior expectations are often used to help students in the general education classrooms, in addition to even more individualized accommodations.
As students prepare to transition out of high school, there are programs to help them get ready for college, job placement, and living independently as an adult.
“It’s really preparing them to live on their own,” Summers said. “It’s really neat to watch the kids go through those stages and really get ready to be totally independent.”
The Superior Alliance for Independent Living also helps with support services and planned activities.
Copper Country Mental Health also offers Applied Behavior Analysis for children with autism (0-21 years old). ABA is an internationally-used approach to teaching skills and changing behaviors, with intense data collection to demonstrate progress and an emphasis on positive reinforcement and practice through repetition. This therapy is available both in the CCMH office and the home, according to Leslie Griffith, CCMH outpatient program director.
Autism and First Responders
Interacting with first responders from the police to firefighters can be a harrowing experience for someone with autism, and difficult for both parties. While a typical child might enjoy seeing firetrucks with the lights and sirens at annual parades, a child with autism is often sensitive to loud sounds and flashing lights and isn’t going to feel comfortable in a parade atmosphere at all. In a tense situation like a car accident or house fire, someone shouting directions or grabbing at a person with autism isn’t likely to get a positive response, either.
For this reason, Summers has been working with a group called Copper Country Autism Awareness Foundation to help kids with autism be more comfortable around first responders and to teach first responders how to recognize and interact with someone who has autism.
Special sensory-sensitive events have been hosted with first responders, at the county fair, and in the emergency room. Flashing lights and loud sounds were disabled, and first responders, nurses, and ER staff were given a chance to interact with local autistic students and their parents without the pressure of an ongoing emergency.
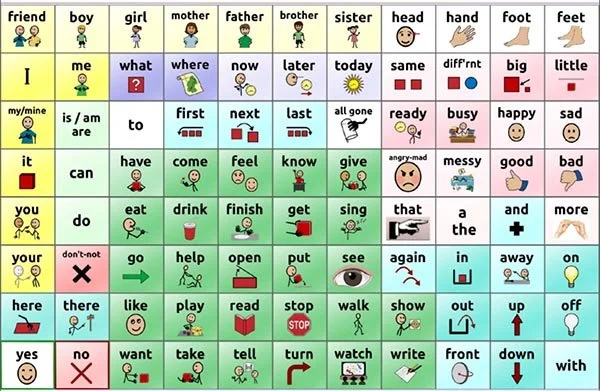
Local first responders have also been equipped with communication tools like a CORE board, which can be used to nonverbally communicate about pain or other emergencies. The emergency room also has weighted blankets and some other things that help soothe anxiety for a child with autism.

An example of a CORE board from praacticalaac.org. Someone who is non-verbal can point at the corresponding images rather than try to speak.
Summers said she has talked with other educators for a long time about trying to bring first responders from across the community to MTU to give classes to them all at once but hasn’t been able to make it happen yet.
Within law enforcement, there’s been a movement toward greater training, too.
“It’s called Managing Mental Health Crisis Training,” Lt. Nick Roberts of the Houghton City Police Department said.
The MMHC training program is approved by the Michigan Commission on Law Enforcement Standards and is developed in cooperation with the National Alliance on Mental Illness. The training is offered by the Cardinal Group II. Roberts and another officer in Houghton are trained instructors in the program, and they work with social workers to train other officers in several departments.
Within the training is a module that focuses on autism and other developmental disorders. Unfortunately, someone with autism or a head injury can sometimes be mistaken by first responders for someone on drugs. The training helps officers recognize telltale signs and behaviors that might indicate that this person actually has a developmental disorder, and teaches them how to interact differently with that person.
“I’m not a professional in autism,” Roberts said.
The training doesn’t enable them to diagnose autism, but there are strategies that can be used in a variety of situations, and officers are taught when to employ them. For instance, Summers said presenting a CORE communications board to someone who doesn’t have autism isn’t likely to produce any helpful results, whereas it likely will if they do have an autism diagnosis. Roberts said focusing on remaining calm, and being mindful of the common autism symptoms like sensitivities to sound and touch are important, as well as tone and body language.
“We can be intimidating,” Roberts said.
He said that’s also why sensory-sensitive events are important, to give everyone a chance to meet first responders outside of an emergency situation. The MMHC training also helps them spot and take advantage of individual opportunities to connect with community members.
“We try to get to know our community,” Roberts said.
In search and rescue situations where someone with autism has gone missing, speed is of the essence.
“Right away, we know it’s going to be a lot more difficult to find that person that can’t communicate,” Roberts said.
Someone with a developmental disorder might also not understand a stranger who finds them is trying to help by pulling at them, or that a loud machine is full of people looking to bring them to safety.
Roberts said encountering someone on the job who is entirely nonverbal is “tough”, but that he always does his best.
“We do have a lot of outcomes that turn out successful because of our training,” he said.
CCAAF did not reply to requests for an interview.
Growing the Supports
Unfortunately, access to these autism supports isn’t always easy.
“Even something like getting a ride to ABA therapy is a barrier for some of our families,” Summers said.
Griffith said CCMH can provide transportation to ABA therapy and other services in cases where no other options are available for the consumer. They’ve also tried to lower other barriers to service like a lack of cellphone minutes when receiving services via the phone, as prepaid and inexpensive cellphone plans often have limited minutes.
Some families can’t afford a car or only have one that’s needed for a parent to commute to work, leaving the other without a way to bring their child to therapy, group activities, and other appointments. Even relatively close sessions could be too distant to get there without a vehicle. Summers said having more local opportunities for therapy in smaller communities, or free transportation services would be helpful for those people.
Summers said another big source of support for people with autism is the CCAAF and wished they could receive more grants.
Summers said the foundation is their “go-to” when they need something in a hurry like an unexpected Lyft or Uber ride to an appointment. They also help with things like specialty support devices, installing safety fences, and helps in other emergencies, too.
“That would be awesome if they had more monies,” Summers said. “Schools just don’t have extra funds.”
Summers said she feels like she could use three more staff members with her training at the CCISD, and her caseload is still growing.
Roberts said he’d like to see more time and money spent on training officers on how to better interact with people with autism, too. He said the pandemic caused many training organizations to move their work online, which helped reduce the necessary travel for local officers to attend sometimes-distant training sessions.
“Zoom saved us a ton of money,” Roberts said.
He thinks the MMHC training should be given to every police officer, and regularly teaches sessions alongside local social workers.
Editor’s note: This story has received multiple updates since its original publishing, on CCMH’s ABA program and available transportation, and correcting how head injuries and autism can be mistaken for drug use.

New programs rising to meet young people’s mental health needs
Local school are implementing tiered systems of support to address the needs of school kids early on.
Tiers of mental and emotional support for students from kindergarten up
A survey of parents conducted by the University of Michigan found that 16.5% of youth between the ages of 6 and 17 experienced a mental health disorder in 2016, but about half of those estimated 7.7 million children went untreated.
In much of Houghton County, there is an overlapping and growing network of programs designed to address the mental health issues of youth as early as possible. They don’t meet every need, but several are newly implemented and seeing positive results even during a tumultuous time.
Many schools are also focusing on mental health supports for students without impairments, or any illness or acute needs at all, too. The idea behind these new programs is to support a student’s mental health needs, starting from basic social support and potentially scaled up to 1-on-1 therapies, as necessary.
Multi-tiered Systems of Support
This is based on Positive Behavioral Interventions and Supports and is being rolled out through the Michigan Department of Education and locally through the intermediate school district. MTSS was launched to take a more proactive approach to identify students with greater needs by first taking a schoolwide approach to basic mental health supports. The program is optional.
“School districts can choose whether or not they have tiered levels of support for students in the schools,” Natalie Morgan said.
Morgan is the mental health services coordinator with the Copper Country Intermediate School District.
Not every school district is involved with MTSS. If districts choose to participate, they create a local team that works with Morgan or another CCISD “coach” to develop and execute the details of their MTSS program.
All students in participating districts are screened and school data is assessed three times throughout the school year. Tiers of support can be escalated to meet an individual or group of student’s needs. Parental involvement is also emphasized.
“We try to have as much communication with parents as we can,” Morgan said.
Sometimes the school can call meetings between a student’s parents, teachers, mental health provider, and even an administrator if necessary, but there are other, positive steps taken first.
“Every student throughout the school gets the tier one supports,” Morgan said.
Tier one - School-wide, foundational work to create a generally structured and supportive atmosphere for students.
This can look different in different schools and classrooms. The structure element comes from the expectations of behavior and conduct.
“So the things that are in, like the student handbook,” Morgan said.
Rather than simply having these posted or distributed, the teacher takes time to teach what the expectations of behavior are.
“Then tier two supports are for those students who just need a little extra boost of those tier one expectations,” Morgan said.
Tier two - Group-level interventions that might include a special reading group or study hall.
These groups can offer some students some extra assistance toward catching up with peers on schoolwork or offer social-emotional learning lessons.
“So that could be friendships, it could be talking about empathy,” Morgan said.
After seeing a lot of missing homework in their data, Baraga High School recently had a homework catch-up day that allowed students to catch up on homework.
“They didn’t tell the students about it at first…” Morgan said. “The percentage of homework completion that was done was like, through the roof.”
Tier two might also include regular 1-on-1 check-ins with teachers throughout the day.
“And it’s not, you know, a 10-minute conversation,” Morgan said. “It’s ‘thanks for sitting down and getting your pencil out right away’ kind of thing.”
Tier three - Individual interventions for students who might need support like 1-on-1 counseling.
“We have a whole range of students who are referred for services,” Morgan said.
Sometimes a student can be referred because of truancy or problem behavior in class, other times it can be because of something that happened at home.
“So it kind of depends on what the school is seeing and how they assess that situation,” Morgan said. “And then a lot of times it’s a referral to services here. To the ISD.”
The CCISD has two full-time and two part-time clinicians to meet referred students with mild to moderate needs. Students with extremely high needs can be referred to Copper Country Mental Health or served by CCISD staff under Project AWARE.
Sessions are usually once a week for 30 to 45 minutes.
Project AWARE
A new program to the area, this program is launched with federal grant dollars from the Substance Abuse and Mental Health Services Administration.
“We technically started it in like January, maybe February of this year,” Morgan said.
Along with some money toward supporting youth mental health treatment, it also funds money toward public education and fighting the stigma surrounding mental health treatment.
One program under this umbrella is Youth Mental Health First Aid. The training is for people like youth pastors, team coaches, and other people who regularly interact with youth.
“It can be employers if they’re an employer that employs youth,” Morgan said.
The training helps someone recognize if a youth is struggling with something and get them any needed support.
DEFINING TRAUMA - A quick sidebar
Trauma is often thought of as something that occurs after a violent or sudden event, like a fire, car crash, or physical abuse.
“It can be that car accident or that one event that happened that’s traumatic,” Morgan said.
But it could also be a divorce or death of a close family member or mentor. There are also complex traumas like generational drug and alcohol abuse or poverty.
“When a traumatic experience happens it can shift how your brain absorbs information,” Morgan said.
The traumatic experience becomes a lens through which the entire world is filtered.
“We see that in soldiers who come back from war,” Morgan said. “If they hear a door slam it can trigger their brain into thinking that is, you know, a gunshot or an explosion of some sort.”
For children, different things can be experienced as traumatic.
“We’ll work with students who have adults in their life who have identified a traumatic experience that the student went through,” Morgan said. “We’ll start working with them and they don’t see it as traumatic.”
When that’s the case, Morgan said they don’t pressure the person to see it as a traumatic event. She said it all depends on how the individual is internalizing an experience. If a person feels it is traumatic, and that memory is impacting how they perceive and react to the world, then therapists work to help them.
Therapy under Project AWARE is with Morgan as a therapist and Andy Kalcich or Allie Richmond, CCISD mental health services specialists, for skill-building. Therapy is where a student might work through trauma or practice mindfulness techniques. In the skill-building portion of their work, they talk about things like what coping skills they use, and each’s respective effectiveness for that individual.
Capturing Kids’ Hearts
Capturing Kids’ Hearts is a program launched by the Flippen Group that also relies on some of the same PBIS science in MTSS, but involves more intensive, direct training for the adults in a school than the state has dedicated for MTSS. CKH particularly focuses on building strong relationships between the students and adults within a school.
Calumet, Laurium and Keweenaw Elementary School recently launched their program locally with grant assistance from the Portage Health Foundation, and this year they were recognized nationally as a model school. It’s only the second year they’ve participated in the program. The selection process includes a direct evaluation as well as surveys from students, parents and staff.
“But the biggest thing to hang our hat on,” Julie Giachino said, “is just the culture we’ve created for these children and staff.”
Giachino is the assistant principal at CLK Elementary School, and one of the school’s first participants in the Flippen Group’s 2-day training. She described the culture transformation as “magical.”
Students are individually greeted as they enter the school building and classrooms.
“You’re engaging that student and finding out--What are their needs, right now?” Darren Kinnunen said.
Kinnunen is the social worker at CLK Elementary. He said a student isn’t going to learn well if they have distractions like needing breakfast or having lost something important to them, or other personal issues. These initial, immediate check-ins are a way to discover those needs and address them before they lead to bigger issues during instruction.

Photo provided by Julie Giachino
One of the first things a class does together at the beginning of the year is create their shared social contract.
“It could be viewed as your set of rules,” Giachino said.
The group develops the classroom rules for the year together, with the teacher leading a discussion about how the students want to be treated, and how the teacher should be treated. Involvement in the process empowers kids to check in on each other, as the rules are shared, rather than just the teacher’s own.
“So anytime there’s conflict or anything in the room… we always go back to that social contract,” Giachino said.
The school staff also develops one for themselves at the beginning of the year. In kindergarten classrooms, they call it the ‘classroom promise’ to keep the vocabulary understandable to the young students.

Two examples of social contracts developed at CLK Elementary this year. The one on the left is from a kindergarten classroom, the one on the right is the staff social contract. Photos provided by Julie Giachino.
Kinnunen said that some instruction time is lost to these extra interactions, but by eliminating distractions and stress students can focus more on academics. He said that Horizons Alternative High School has found more classes are being completed since they’ve started spending time implementing Capturing Kids’ Hearts.
“Once you have their heart, their minds are open,” Giachino said.
The concepts of CKH are along the same guidelines at Tier one MTSS supports. The program also dovetails with other programs CLK Elementary has enacted in the last couple of years.
KINGS Time
Through each week, the CLK Elementary School’s social worker, Kinnunen, spends 40 minutes with each class talking about things like problem-solving, developing empathy, understanding your own emotions, and social interaction.
“Some kids are maybe getting it at home, right?” Kinnunen said. “Just because of the household that they have. Some kids aren’t getting it.”
It also helps Kinnunen build a rapport with the kids so that if they come in to see him about an individual problem, they already have the basis of a mentor-mentee relationship.
“For me, it’s just a great opportunity to connect with kids,” Kinnunen said.
These social classes are also very similar to some Tier two MTSS supports, but enacted across the entire elementary school rather than targeted.
Therapy Dogs
Benny the therapy dog and Matt Hampton, CLK Elementary principal. Photo by Joshua Vissers
The CLK district currently has five hypoallergenic therapy dogs that spend their days at the schools. Two are in the elementary school. Sometimes they’re scheduled to be in classrooms, other times they’re in one-on-one meetings.
“He even comes in here once in a while for some of our parent meetings and he’ll jump over there on the chair,” Matt Hampton, CLK Elementary School principal, said. “It really not only puts students at ease but also puts parents at ease.”
Right now the new dogs are training with Hampton and waiting for programs to restart after the pandemic. The dogs that have been in the building longer went through Pet Partners training.
“It’s been a great success for us,” Kinnunen said.
Handle With Care
CLK Schools have coordinated with local police in this state program to increase their awareness of what students are experiencing outside of school.
“We recognized that there are some students in our district that may have been affected by just, trauma, in their life,” Kinnunen said, “and that maybe we weren’t picking up on some of that.”
Kinnunen would sometimes find that students in his office had major events happen in their lives that the school staff was completely in the dark about.
In the Handle With Care program, if police encounter schoolkids when on a call, they inform the school; not of all the details, but simply that the student may be tired from lack of sleep, distracted in class by something that happened, or need extra support temporarily.
“Depending on the circumstance, it might just be a check-in and not really talk about what happened last night,” Kinnunen said. “But just to say ‘Hey, how are you doing?’”
It’s a simple program, conducted via email, and Kinnunen highly recommends it to other districts.
Copper Country Mental Health
In addition to assisting schools with many of the above programs and being directly involved with Project AWARE, Copper Country Mental Health also provides several independent programs.
“We provide a whole array of services, as required by the Michigan Department of Health and Human Services,” said CCMH Executive Director Cari Raboin.
Much of their programs are paid for through Medicaid, which sets a severity condition on the treatment they can offer and requires them to follow other MDHHS rules, too.
Independent referrals go through NorthCare Network. Most children need a parent or legal guardian involved, but there are some limited services available without parental consent to those over the age of 14.
Leslie Griffith is the outpatient program director at Copper Country Mental Health, but spent 17 years of her career focused on early childhood and youth treatment, a segment of the population she says are particularly underserved.
CCMH considers youth to be prenatal to age 21.
Griffith wrote in an email that the goal of youth intervention programs is to reduce problematic behaviors and symptoms to ultimately have “a decrease in functional impairment”. Functional impairment is simply the barriers or limitations an illness places on carrying out a person’s daily life.
Services can be paid for through some private insurance, Medicaid, or MiChild insurance, according to Griffith. Charges are also income-adjusted.
“I’m concerned that people aren’t calling us who are eligible for our services,” Raboin said.
She said anyone in doubt of their need or financial assistance eligibility should call 1-888-906-9060 for a screening.
Parent Support Partner
PSP is a program to help parents with training and support to be caretakers of children with serious emotional disturbances. The goal is to move families to independence from counselors and other interventions through training in how to directly participate in the treatment process.
Youth Peer Support Services
This program pairs youth with a young adult to offer advice and support.
Wraparound
This program helps coordinate the supportive adults in the orbit of a child who has serious emotional disturbance to have a team approach in managing the necessary support. The program is especially effective for those involved with multiple institutions.
A variety of education and training programs.
Dial Help
A local organization originally established to address addiction, Dial Help now offers a variety of support services.
Crisis Line
To talk to someone about available help and resources in the community, Dial Help keeps someone available around the clock. They offer specialized youth services and can make referrals to other experts.
Call: 1-800-562-7622
Text: 906-356-3337
Dial Help supports the local Communities That Care initiative, which uses an evidence-based prevention model to address youth substance abuse, delinquency, and mental health. The organization relies heavily on volunteers.
Pandemic’s impact on youth mental health
“There’s definitely been some ups and downs,” Morgan said.
One of the positives, according to her, is that insurance companies and other institutions have come to recognize the value and effectiveness of teletherapy, which is conducting therapy sessions via video conferencing.
“Some of those students who have been virtual, we’ve done virtual sessions with them,” Morgan said.
She said more people have been able to participate in meetings virtually, too.
On the other hand, the distance has created some problems, too.
“If a student doesn’t want to meet, they just don’t log on,” Morgan said.
Morgan said the pandemic exacerbated the anxiety and depression some students they see were already feeling.
“So it’s just being able to recognize that and really working with students on different coping skills and things that they can use to kind of help get through this,” Morgan said.
The CCISD staff has been approved to keep meeting with students into the summer.
At CLK Elementary, the challenge was how to continue connecting with students when schools went virtual. CLK Elementary was only closed twice in the last school year, both in the fall, but the staff said switching back and forth was difficult.
Social contracts and regular greetings continued, but the venue changed.
Kinnunen said that they tried to maintain what schedule consistency they could so that students could develop new habits.
“We’re all creatures of habit, right?” he said. “Anytime there’s a shift, it just throws your system.”
Kids that didn’t show up for classes got calls from paraprofessionals and other staff from the school to check in on why.
The change to virtual learning also presented some students with issues finding both devices and internet access to participate. Different solutions were found for each, with the Portage Health Foundation assisting with establishing wifi hotspots, too.
Struggling to meet community staffing needs
“It’s mostly just qualified therapists to provide the services,” Morgan said.
Morgan said the CCISD has been fortunate in their hiring, but other ISDs in the UP have struggled just to find qualified people to fill those positions, and keep them there.
Currently, the CCISD has a small staff serving several school districts, with more joining the MTSS program. Morgan said more support from within the individual school districts would be very helpful. Social workers in schools, like Kinnunen, are beginning to be more common.
“If we could have, you know, be able to provide a social worker in every school, that would be phenomenal,” Morgan said.
Griffith wrote that there are “certainly” unaddressed needs in the community, but that families with higher income have access to private practitioners.
Raboin also said staffing is an issue. CCMH covers a four-county area with a small staff that has to be able to do many different things.
“Our staff really have to be jacks of all trades,” Griffith said.
Frequent turnover makes keeping well-trained people on the job difficult. The geographic differences across the state aren’t always accounted for in the requirements they’re placed under, and encouraging needed people to move to the area isn’t always easy, either.
Social workers and therapists have specific educational requirements that have to be met as well. Raboin said CCMH has found success using remote teletherapy for their patients, as then therapists can be non-local.